Cephalosporins and Cephalosporin/β-Lactamase Inhibitor Combinations
Cephalosporins and
Cephalosporin-β-Lactamase Inhibitors
Russell E. Lewis
Associate Professor of Infectious Diseases
Department of Molecular Medicine
University of Padua

russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.idpadova.com
Discovery of cephalosporins:
From Sardinian sewage to modern medicine
1945: Giuseppe Brotzu discovers antimicrobial activity
- Epidemiologist working in Sardinia, Italy
- Isolated Cephalosporin acremonium from sewage outflow
- Demonstrated activity of filtrate against gram-positive AND gram-negative bacteria
- Could not find resources from Italian government to develop antibiotic- sent to UK where cephalosporin C was isolated in the 1950s
Amazing fact
Brotzu noticed that locals who swam near sewage outfalls rarely developed typhoid fever, leading to his investigation. It took almost two decades from discovery to clinical use (1964)!
Basic cephem nucleus
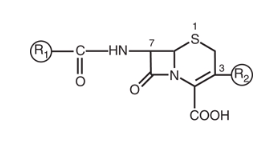
Core structure:
- β-lactam ring fused to a 6-member dihydrothiazine ring
- Starting material: 7-aminocephalosporanic acid (7-ACA)
Key difference from penicillins:
- Penicillin: 5-member thiazolidine ring
- Cephalosporin: 6-member dihydrothiazine ring
R1 Modifications: Enhancing spectrum
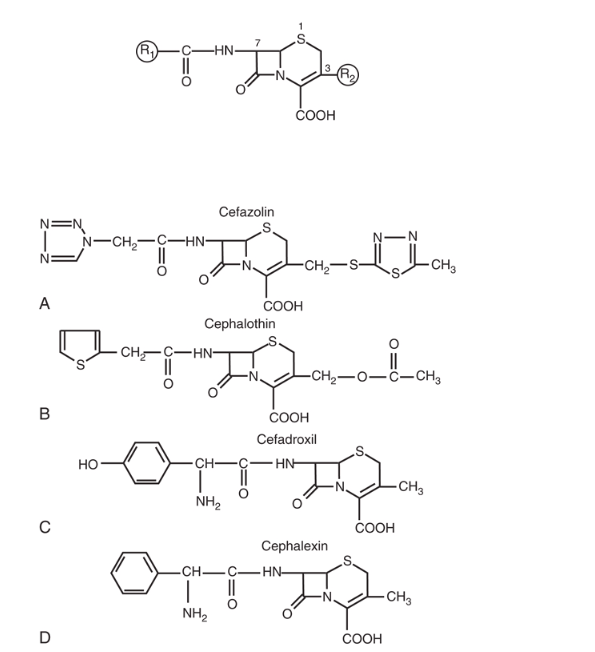
α-Carbon modifications at C7:
- Hydroxyl group → Enhanced gram-negative (cefuroxime)
- Methoxyimino group → 3rd generation spectrum
- 2-Aminothiazol group → 3rd/4th generation potency
Cephamycins
Methoxy substitution at C7 → Cefoxitin, Cefotetan
Enhanced anaerobic coverage
Resistance to many β-lactamases
BUT: Reduced gram-positive activity
Second generation cephalosporins
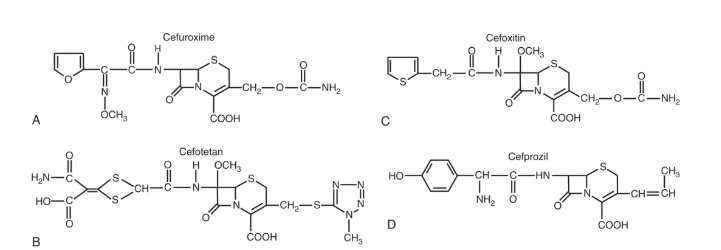
Available agents:
- IV: Cefuroxime, Cefoxitin, Cefotetan
- PO: Cefuroxime axetil, Cefaclor, Cefprozil
Enhanced coverage:
Better H. influenzae activity
Cephamycins: Bacteroides fragilis coverage
Third generation cephalosporins
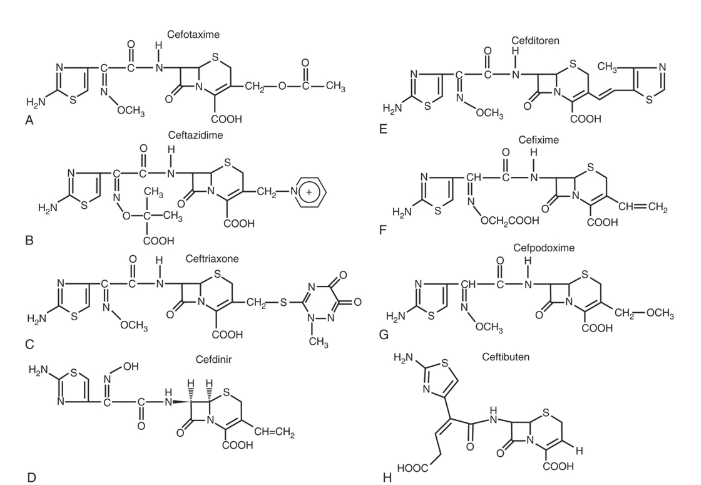
Parenteral agents:
- Ceftriaxone (once daily - long half-life)
- Cefotaxime (CNS penetration)
- Ceftazidime (Pseudomonas activity)
Oral agents:
- Cefixime, Cefpodoxime, Cefdinir, Ceftibuten
Key features:
- Significantly enhanced gram-negative coverage
- Most penetrate CNS with inflamed meninges
- Reduced gram-positive activity (except ceftriaxone)
Fourth generation: Cefepime
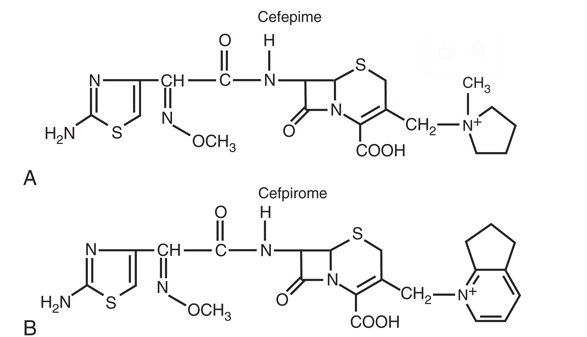
Key advantages:
- Zwitterionic structure → Rapid outer membrane penetration
- Enhanced stability against AmpC β-lactamases
- Maintains Pseudomonas activity
- BETTER gram-positive coverage than ceftazidime
- Good CNS penetration (also risk of neurotoxicity in renal impairment > 20–22 mg/L due to GABA-A antagonism)
Dosing: 1-2 g IV q8-12h
Fifth generation: Ceftaroline
FDA-approved indications:
- Acute bacterial skin and skin structure infections (ABSSSI)
- Community-acquired bacterial pneumonia (CABP)
Limitations:
- NO activity against Pseudomonas
- NO activity against ESBL-producers
- Parenteral only (600 mg IV q12h)
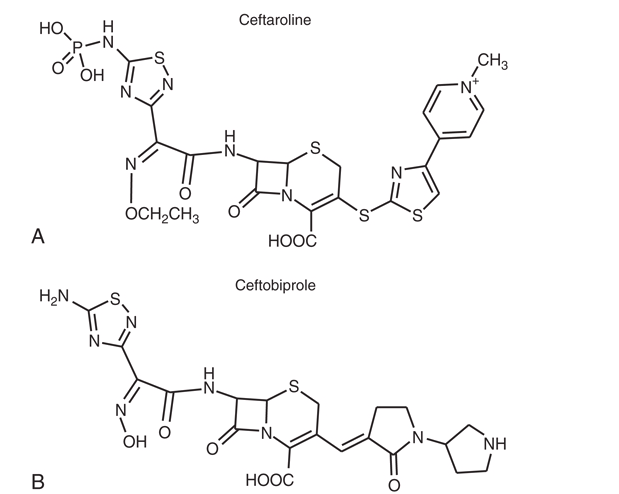
Anti-MRSA Activity
Ceftaroline binds to PBP2A → Activity against MRSA
Ceftolozane-tazobactam
Structure: Novel cephalosporin + tazobactam
Key features:
- Excellent activity against P. aeruginosa (including MDR)
- Active against ESBL-producing Enterobacterales
- Intrinsic AmpC stability
Limitations
NO activity against:
- KPC-producing organisms
- Metallo-β-lactamase (MBL) producers
- OXA-48 producers
Dosing:
1.5-3 g IV q8h
Extended infusion 3 g (over 3 h) q8h or LD 3 gram and 9 grams (over 24h) daily
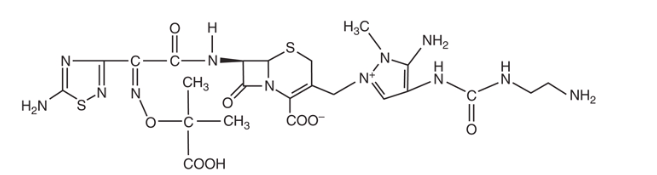
Cefiderocol: Siderophore cephalosporin
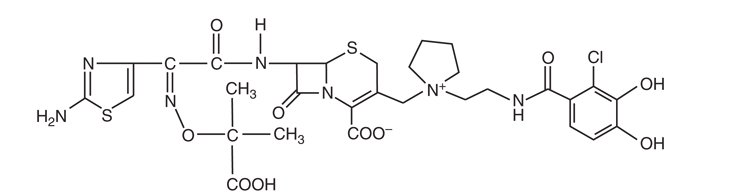
“Trojan Horse” Mechanism
- Contains catechol moiety that binds iron
- Hijacks bacterial iron transport systems
- Delivers cephalosporin directly into cell
Unique spectrum:
- Active against MBL-producers (NDM, VIM, IMP)
- Acinetobacter baumannii complex
- Stenotrophomonas maltophilia
- Carbapenem-resistant Enterobacterales
Dosing: 2 g IV q8h (3-hour infusion)