Aminoglycosides
Aminoglycosides
Russell E. Lewis
Associate Professor of Infectious Diseases

russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.idpadova.com
Learning Objectives
By the end of this lecture, you will be able to:
- Describe the mechanism of action and pharmacodynamic properties
- Compare the spectrum of activity among aminoglycoside agents
- Apply weight-based and renal-adjusted dosing strategies
- Identify patients at risk for nephrotoxicity and ototoxicity
- Design appropriate therapeutic drug monitoring plans
- Select appropriate aminoglycosides for specific clinical scenarios
Lecture outline
Part 1: Fundamentals
- History & discovery
- Chemical structure
- Mechanism of action
- PK/PD principles
Part 2: Clinical application
- Spectrum & Resistance
- Dosing Strategies
- Adverse Effects
- Therapeutic Monitoring
- Clinical Scenarios
PART 1: Fundamentals
Historical Timeline
| Year | Discovery |
|---|---|
| 1944 | Streptomycin (first aminoglycoside) |
| 1949 | Neomycin |
| 1957 | Kanamycin |
| 1963 | Gentamicin |
| 1967 | Tobramycin |
| 1972 | Amikacin |
| 2018 | Plazomicin |
The discovery of streptomycin
- 1943-1944: Selman Waksman’s laboratory at Rutgers
- Systematic screening of soil actinomycetes
- Isolated from Streptomyces griseus
- First effective treatment for tuberculosis
- Ringo Starr (Beatles drummer) among first treated patients!
- Waksman awarded Nobel Prize (1952)
“The grueling search through 10,000 soil samples yielded streptomycin”

Nomenclature convention
“-mycin” suffix
- Derived from Streptomyces species
- Examples: Streptomycin, Neomycin, Kanamycin, Tobramycin
“-micin” suffix
- Derived from Micromonospora species
- Examples: Gentamicin, Sisomicin, Plazomicin
Currently FDA-approved agents
| Agent | Year | Primary Use |
|---|---|---|
| Gentamicin | 1963 | Gram-negative infections, synergy |
| Tobramycin | 1967 | Pseudomonas, CF |
| Amikacin | 1972 | Resistant gram-negatives, TB |
| Plazomicin | 2018 | CRE, MDR organisms |
Streptomycin: Limited availability (TB, plague, tularemia)
Family of aminoglycosides in clinical use
| Generic Name | Proprietary Name | Source | Year Reported | Chemistry |
|---|---|---|---|---|
| Streptomycin | None | Streptomyces griseus | 1944 | Unique central aminocyclitol ring |
| Neomycin | Mycifradin, Neobiotic | Streptomyces fradiae | 1949 | Roughly equal proportions of neomycin B and C |
| Kanamycin | Kantrex | Streptomyces kanamyceticus | 1957 | Mixture of 95% kanamycin A and 5% kanamycin B |
| Paromomycin | Humatin | S. fradiae | 1959 | Part of neomycin family |
| Spectinomycin | Trobicin | Streptomyces spectabilis | 1961 | Chemically distinct but closely related to aminoglycosides |
| Gentamicin | Garamycin | Micromonospora purpurea and Micromonospora echinospora | 1963 | Roughly equal proportions of gentamicin C₁, C₁ₐ, and enantiomers C₂ and C₂ₐ |
Chemical structure overview
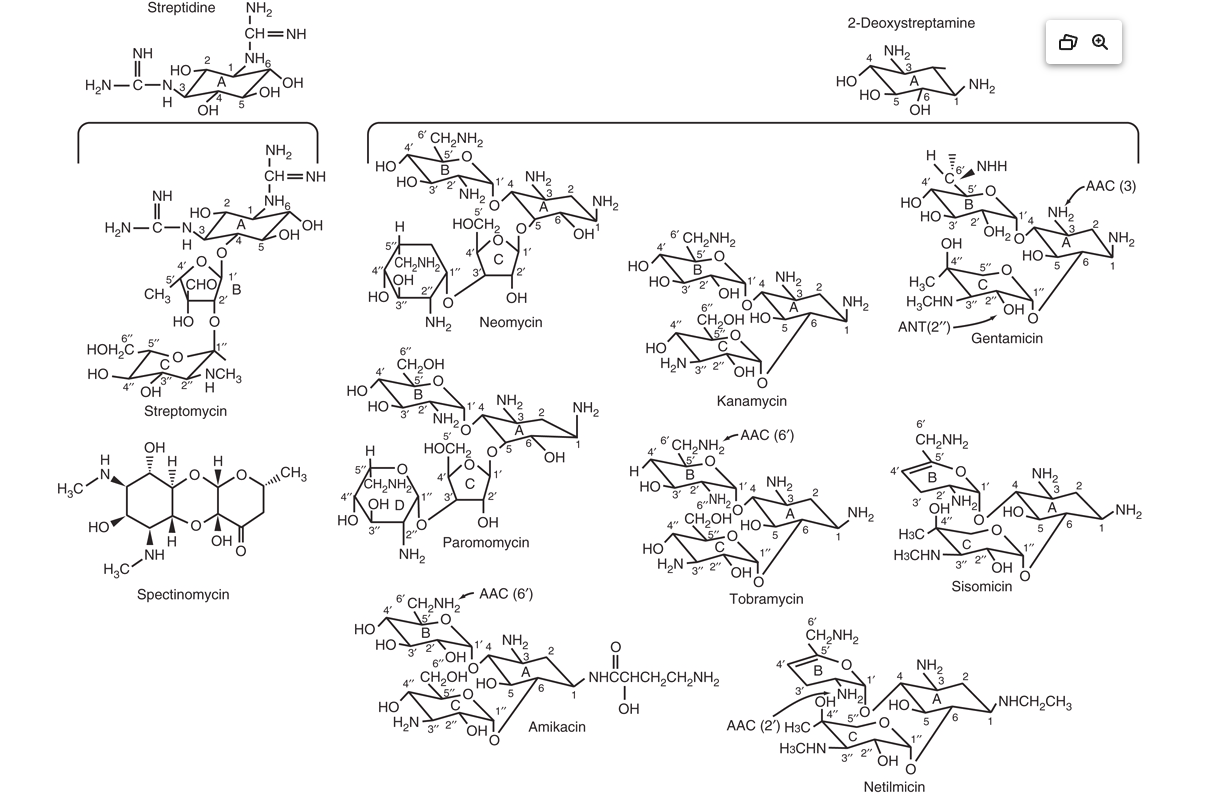
Structural classification
Streptidine-containing:
- Streptomycin (unique structure)
2-Deoxystreptamine (4,5-disubstituted):
- Neomycin, Paromomycin
2-Deoxystreptamine (4,6-disubstituted):
- Kanamycin, Amikacin, Tobramycin
- Gentamicin, Sisomicin, Plazomicin
Key chemical properties
- Polycationic at physiological pH
- Highly polar (water soluble)
- Heat stable
- Not absorbed orally (< 1%)
- Not metabolized (excreted unchanged)
These properties directly influence:
- Distribution (limited to extracellular fluid)
- Elimination (renal, GFR-dependent)
- Drug interactions (binding to cell membranes)
Aminoglycosides:MOA
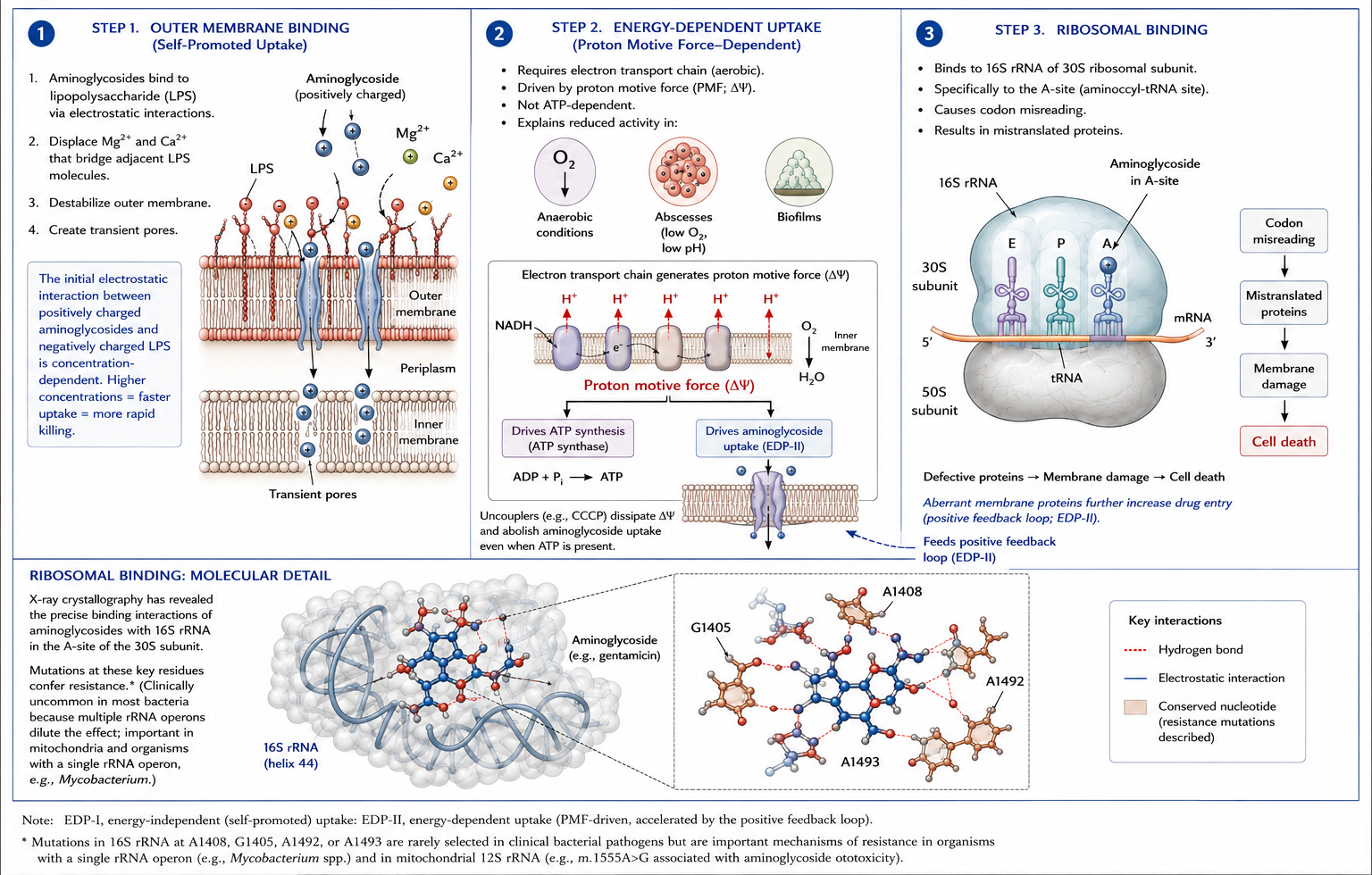
Why aminoglycosides are bactericidal
Unique among ribosomal inhibitors:
| Drug Class | Target | Effect |
|---|---|---|
| Aminoglycosides | 30S | Bactericidal |
| Tetracyclines | 30S | Bacteriostatic |
| Macrolides | 50S | Bacteriostatic |
| Linezolid | 50S | Bacteriostatic |
Reason: Mistranslated membrane proteins cause irreversible damage
Concentration-dependent killing
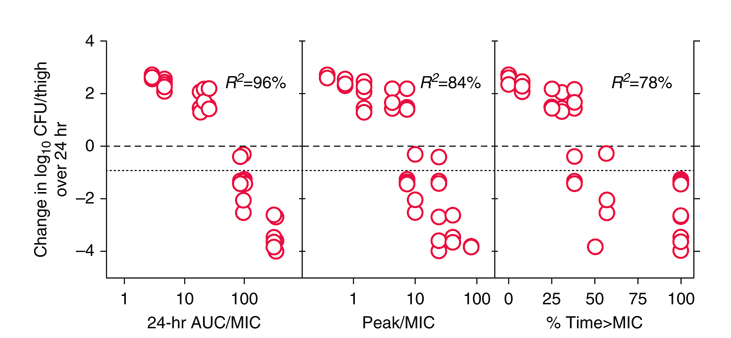
Higher peak concentrations = Greater bacterial kill
Post-Antibiotic Effect (PAE)
Definition: Continued suppression of bacterial growth after drug removal
Duration: 3-8 hours for gram-negative bacteria
Clinical implication: Supports extended-interval dosing
| Organism | Approximate PAE |
|---|---|
| E. coli | 2-4 hours |
| P. aeruginosa | 2-6 hours |
| S. aureus | 3-6 hours |
PK/PD target parameters
Historical target:
- Cmax/MIC ratio ≥ 8-10
Current understanding:
- AUC/MIC is primary efficacy driver
- Target AUC/MIC: 80-120 (organism-dependent)
For extended-interval dosing:
- Target peak: 15-20 mg/L (gentamicin/tobramycin)
- Target peak: 56-64 mg/L (amikacin)
- Target trough: Undetectable (< 1 mg/L)
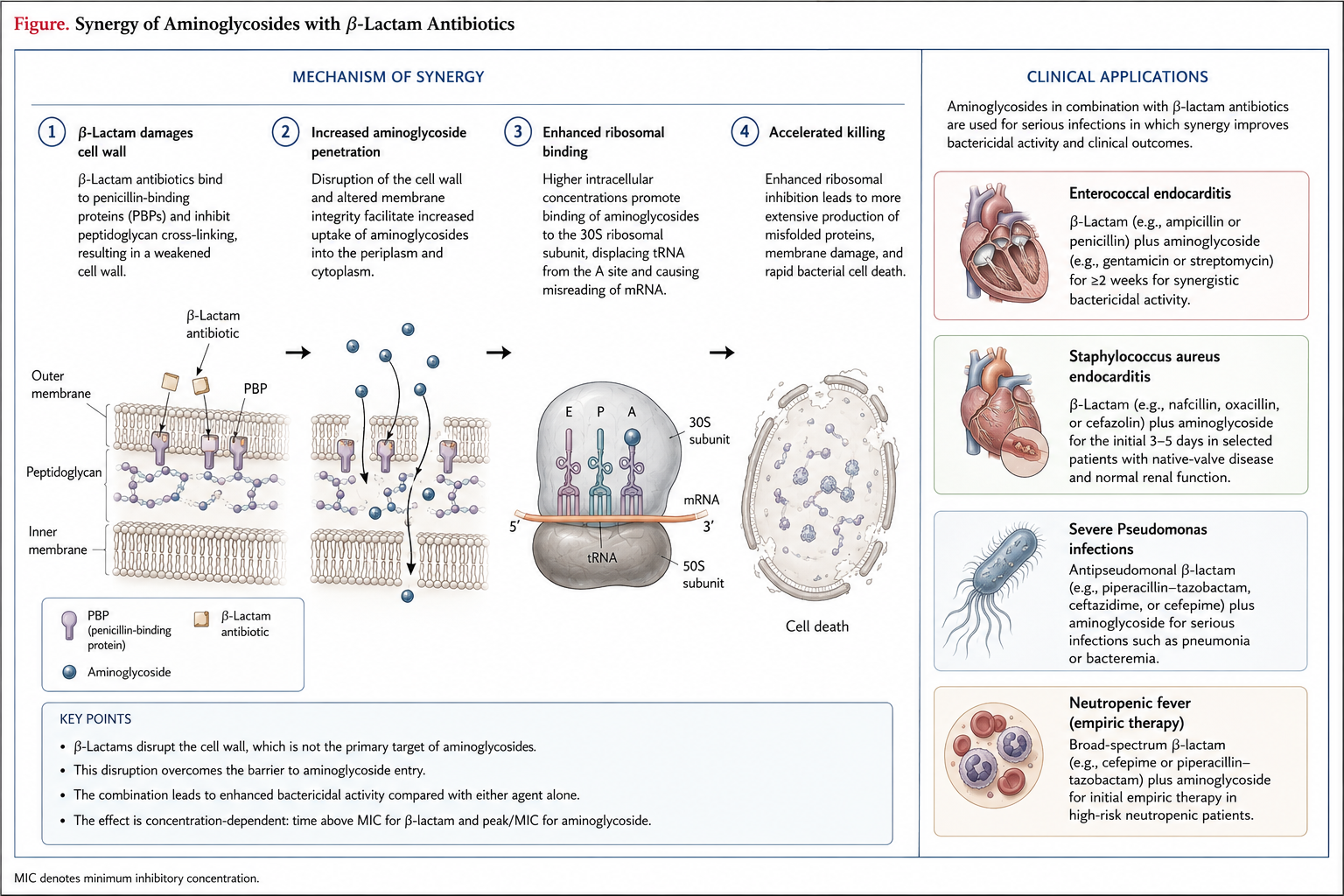
Synergy with β-lactams
PART 2: Clinical Application
Spectrum of activity: Overview
Good activity:
- Enterobacteriaceae
- Pseudomonas aeruginosa
- Staphylococcus spp.
- Mycobacterium spp.
Limited/No activity:
- Anaerobes
- Streptococci (except synergy)
- Stenotrophomonas
- Most Acinetobacter
Agent selection by organism
| Organism | Preferred Agent |
|---|---|
| P. aeruginosa | Tobramycin > Amikacin |
| Enterobacteriaceae | Gentamicin = Tobramycin |
| Resistant gram-negatives | Amikacin |
| CRE | Plazomicin > Amikacin |
| MRSA (synergy) | Gentamicin |
| Enterococci (synergy) | Gentamicin |
| M. tuberculosis | Streptomycin, Amikacin |
Plazomicin: Overcoming resistance
Designed to evade:
- Aminoglycoside-modifying enzymes (AMEs)
- Most common resistance mechanism
Active against:
- CRE (carbapenem-resistant Enterobacteriaceae)
- ESBL producers
- Most aminoglycoside-resistant strains
Limitations:
- Inactivated by 16S rRNA methyltransferases
- More expensive than legacy agents
Resistance mechanisms

Clinical indications
Primary indications (usually combination therapy):
- Sepsis/septic shock
- Hospital-acquired/ventilator-associated pneumonia
- Complicated intra-abdominal infections
- Complicated urinary tract infections
- Neutropenic fever
- Infective endocarditis
Additional clinical uses
- Tuberculosis (MDR-TB regimens)
- NTM infections (MAC, M. abscessus)
- Surgical prophylaxis (GI/GU procedures)
- Orthopedic cement (arthroplasty)
- Ophthalmic infections (topical)
- Cystic fibrosis (inhaled tobramycin)
- Selective digestive decontamination
Endocarditis: Synergy dosing
Enterococcal endocarditis:
- Ampicillin + Gentamicin
- Gentamicin 3 mg/kg/day divided q8h
- Duration: 4-6 weeks (gent for 2-4 weeks)
- Check for high-level resistance (MIC > 500)
Staphylococcal endocarditis (native valve):
- Optional gentamicin × 3-5 days
- Controversial benefit vs. toxicity risk
Empiric therapy: Neutropenic fever
Traditional regimen:
- Anti-pseudomonal β-lactam + aminoglycoside
Current guidelines (IDSA 2010):
- Monotherapy often sufficient (cefepime, piperacillin-tazobactam, anti-pseudomonal carbapenem)
- Add aminoglycoside if:
- Hemodynamic instability
- Suspected resistant gram-negative
- High local resistance rates
Dosing Strategies
Extended-interval vs. Traditional dosing
| Feature | Extended-Interval | Traditional |
|---|---|---|
| Frequency | q24h | q8-12h |
| Peak | Higher | Lower |
| Trough | Undetectable | Detectable |
| Efficacy | Optimized | Adequate |
| Toxicity | Lower | Higher |
| Monitoring | Simpler | Complex |
Extended-interval is preferred for most indications
Extended-Interval Dosing Regimens
| Agent | Dose | Frequency |
|---|---|---|
| Gentamicin | 5-7 mg/kg | q24h |
| Tobramycin | 5-7 mg/kg | q24h |
| Amikacin | 15-20 mg/kg | q24h |
| Plazomicin | 15 mg/kg | q24h |
Use actual body weight unless obese
Traditional dosing (Synergy)
| Agent | Daily Dose | Division |
|---|---|---|
| Gentamicin | 3 mg/kg/day | q8h or q12h |
| Tobramycin | 3 mg/kg/day | q8h or q12h |
Target peaks: 3-4 mg/L
Target troughs: < 1 mg/L
Used for:
- Enterococcal endocarditis
- Staphylococcal endocarditis (if used)
- Gram-positive synergy
Dosing in obesity
Definition of obesity for dosing:
- Actual weight > 120% of ideal body weight, OR
- BMI ≥ 30 kg/m²
Calculate adjusted body weight (ABW):
\[ABW = IBW + 0.4 \times (Actual - IBW)\]
Ideal body weight (IBW):
- Males: 50 kg + 2.3 kg per inch over 5 feet
- Females: 45.5 kg + 2.3 kg per inch over 5 feet
Obesity dosing example
Patient: 180 kg male, 5’10” (70 inches)
Step 1: Calculate IBW \[IBW = 50 + 2.3(70-60) = 73 kg\]
Step 2: Calculate ABW \[ABW = 73 + 0.4(180-73) = 73 + 42.8 = 115.8 kg\]
Step 3: Calculate dose \[Gentamicin = 7 mg/kg \times 116 kg = 812 mg\]
Round to 800 mg IV q24h
Dosing in renal impairment
Key principle: Aminoglycoside clearance ≈ GFR
| CrCl (mL/min) | Interval Adjustment |
|---|---|
| > 60 | q24h |
| 40-60 | q36h |
| 20-40 | q48h |
| < 20 | Extend further or use TDM |
Alternative: Reduce dose, maintain interval
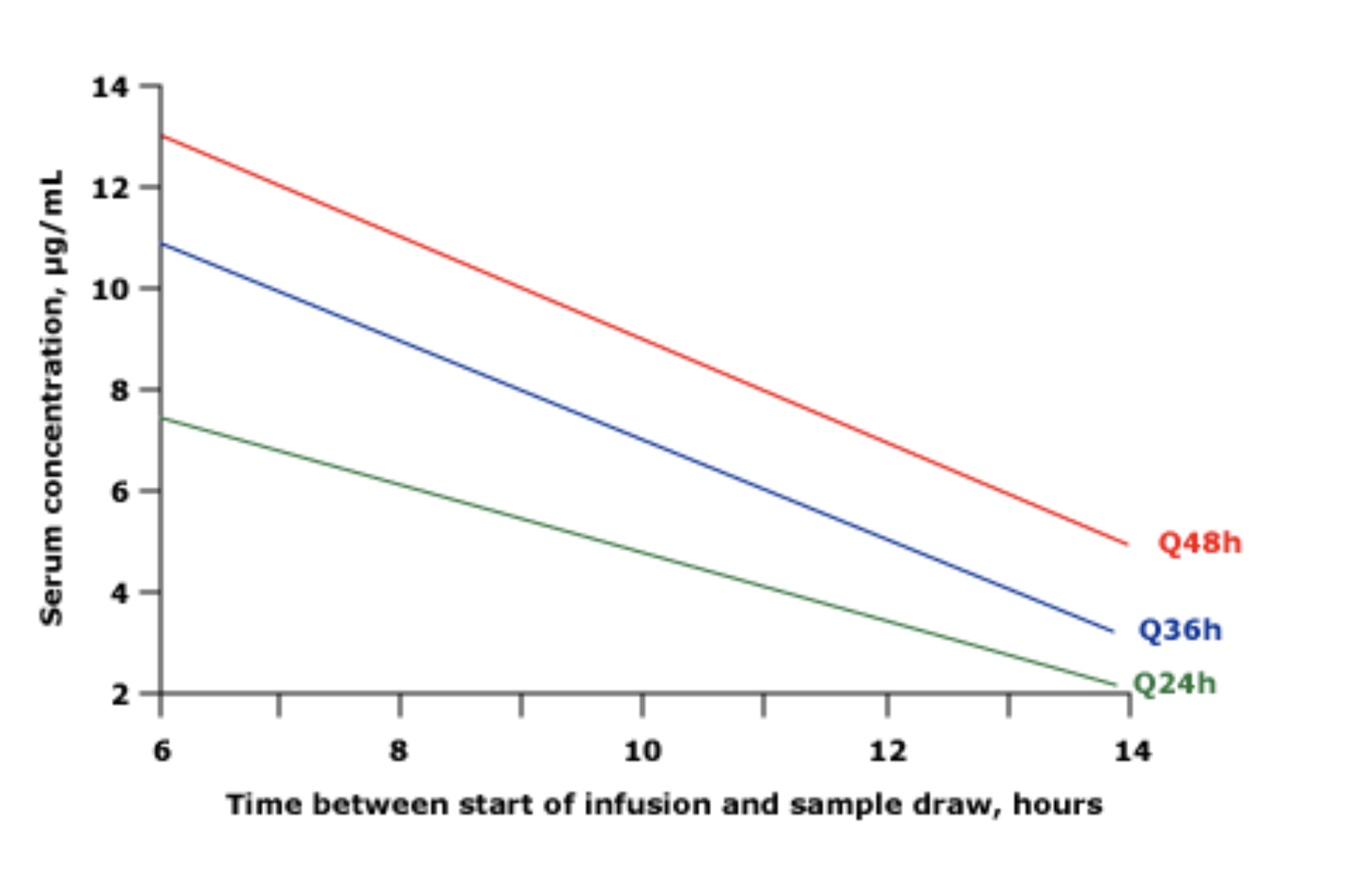
Renal dosing: Hartford nomogram
For gentamicin/tobramycin 7 mg/kg:
- Give first dose based on weight
- Draw level at 6-14 hours post-dose
- Plot on nomogram
- Determines q24h, q36h, or q48h dosing
Advantages:
- Simple
- Single level needed
- Validated in clinical trials
Extended-interval- monitoring
Hartford nomogram
Hemodialysis dosing
Conventional hemodialysis:
- Dose q48-72h (non-dialysis days)
- Give after dialysis
- OR give 50% supplemental dose post-dialysis
High-flux hemodialysis:
- Greater drug removal
- May need larger supplemental doses
- TDM essential
Measure levels to guide dosing
CRRT dosing
Continuous renal replacement therapy:
- Drug clearance ≈ effluent rate
- Typical: CrCl equivalent of 10-50 mL/min
- Use standard doses with extended intervals (q24-48h)
- TDM mandatory
| CRRT Mode | Typical Clearance |
|---|---|
| CVVH | 15-25 mL/min |
| CVVHD | 20-30 mL/min |
| CVVHDF | 25-40 mL/min |
Adverse Effects
Toxicity overview
Dose-limiting toxicities:
- Nephrotoxicity (5-25% incidence)
- Ototoxicity (2-10% incidence)
- Neuromuscular blockade (rare)
Risk increases with:
- Duration of therapy
- Total cumulative dose
- Elevated trough concentrations
- Concurrent nephrotoxins
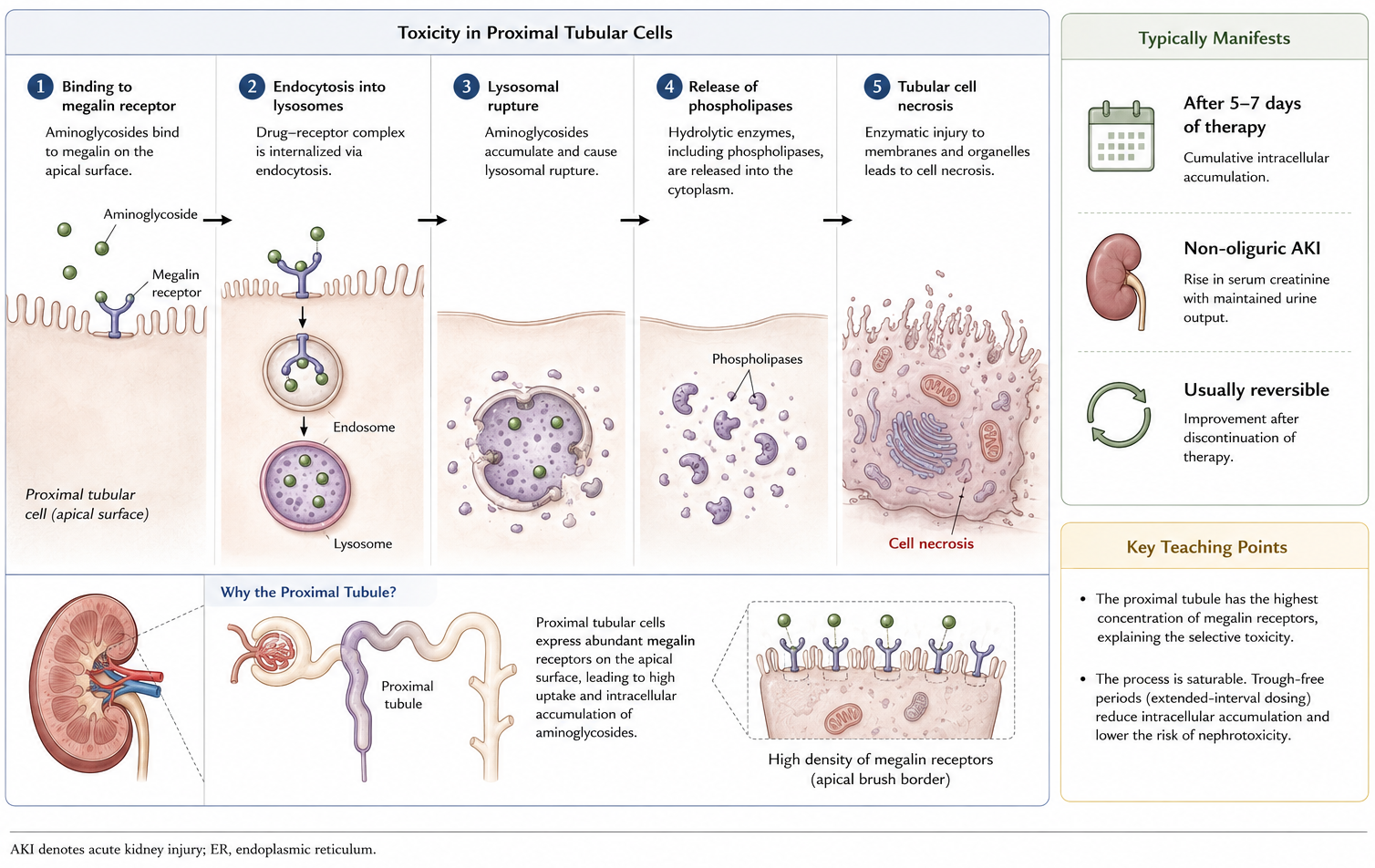
Nephrotoxicity: mechanism
Nephrotoxicity: Risk factors
Patient factors:
- Pre-existing renal disease
- Advanced age
- Volume depletion
- Hypotension
Drug factors:
- Duration > 5-7 days
- Elevated trough concentrations
- Total cumulative dose
- Concurrent nephrotoxins
Concurrent nephrotoxins:
- Amphotericin B, vancomycin, NSAIDs
- IV contrast, cisplatin, cyclosporine
Preventing nephrotoxicity
Use extended-interval dosing
- Drug-free intervals reduce accumulation
Keep courses short (≤5 days when possible)
Monitor troughs
- Target: Undetectable (< 1 mg/L)
Maintain euvolemia
Avoid concurrent nephrotoxins when possible
Monitor serum creatinine every 2-3 days
Ototoxicity: Two forms
Cochlear toxicity (hearing loss):
- High-frequency hearing loss first
- May progress to speech frequencies
- Often irreversible
- Associated with: amikacin, kanamycin, neomycin
Vestibular toxicity:
- Vertigo, nystagmus, ataxia
- May improve with time/compensation
- Associated with: gentamicin, streptomycin, tobramycin
Ototoxicity: mechanism
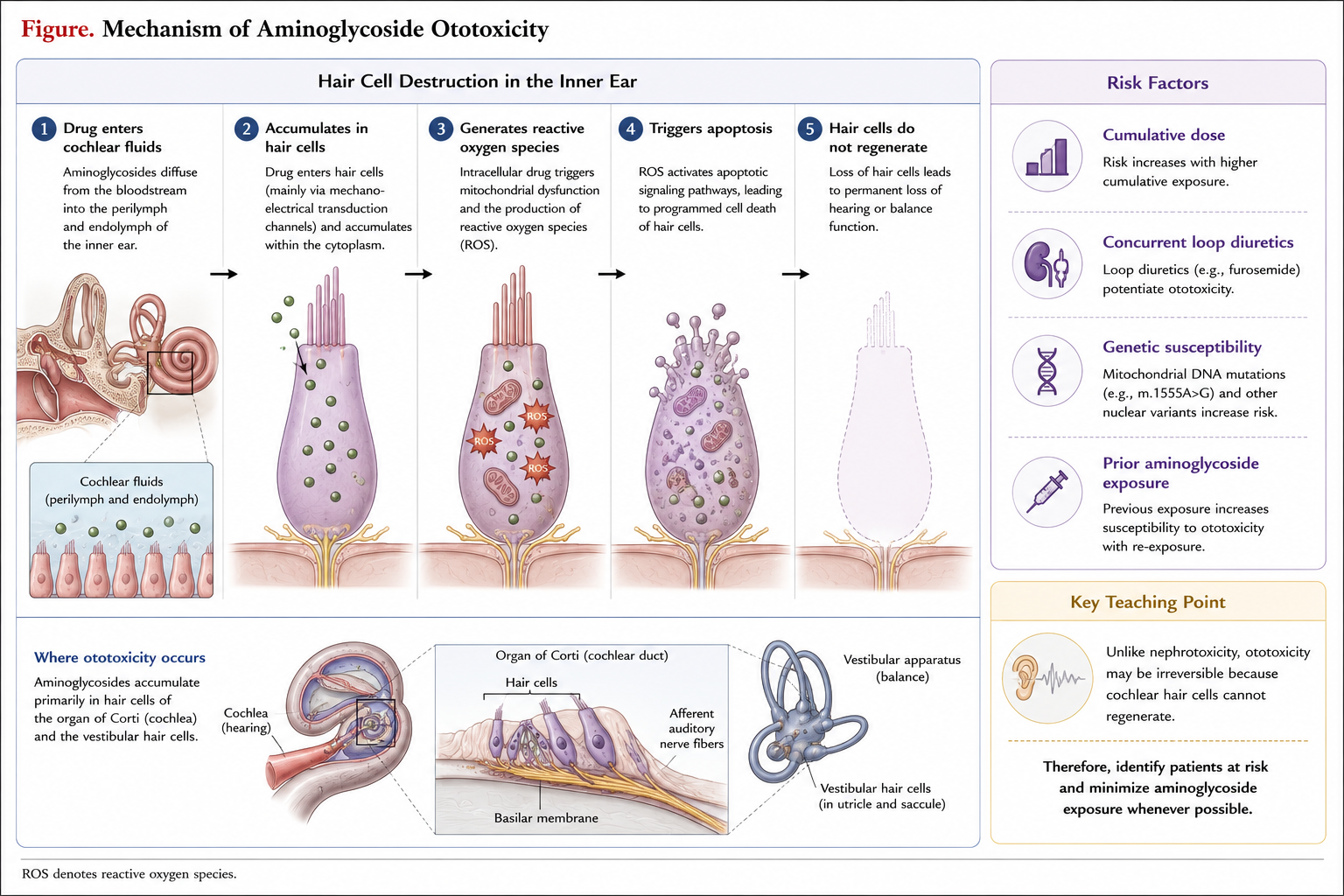
Genetic risk: MT-RNR1 mutation
m.1555A>G mitochondrial mutation:
- Prevalence: ~1 in 500 individuals
- Makes mitochondrial ribosome resemble bacterial ribosome
- Single dose can cause permanent deafness
Implications:
- Point-of-care testing available
- Being implemented for neonatal screening
- Family history of aminoglycoside-induced deafness
Neuromuscular blockade
Mechanism:
- Inhibition of presynaptic acetylcholine release
- Blockade of postsynaptic receptor
Risk factors:
- Myasthenia gravis
- Concurrent neuromuscular blockers
- Hypocalcemia, hypomagnesemia
- Rapid IV infusion
Management:
- Calcium gluconate
- Neostigmine (limited efficacy)
Drug interactions
| Interacting Drug | Effect |
|---|---|
| Amphotericin B | ↑ Nephrotoxicity |
| Vancomycin | ↑ Nephrotoxicity |
| Loop diuretics | ↑ Ototoxicity |
| Cisplatin | ↑ Both toxicities |
| Neuromuscular blockers | ↑ Paralysis |
| NSAIDs | ↑ Nephrotoxicity |
| IV contrast | ↑ Nephrotoxicity |
Therapeutic Drug Monitoring
When is TDM Needed?
Always recommended:
- Therapy > 3-5 days
- Renal impairment (any degree)
- Critical illness
- Obesity
- Burns
- Pregnancy
- Elderly patients
Optional (short course, normal renal function):
- Duration ≤ 3 days
- Stable patients
Peak and trough Targets
Extended-interval dosing:
| Agent | Target peak | Target trough |
|---|---|---|
| Gentamicin | 15-20 mg/L | < 1 mg/L |
| Tobramycin | 15-20 mg/L | < 1 mg/L |
| Amikacin | 56-64 mg/L | < 5 mg/L |
Traditional dosing (synergy):
| Agent | Target peak | Target trough |
|---|---|---|
| Gentamicin | 3-4 mg/L | < 1 mg/L |
Sample timing approaches
Peak level:
- Draw 30-60 minutes after end of infusion
- Ensures distribution phase complete
Trough level:
- Draw within 30 minutes before next dose
Two-level kinetics:
- Both samples in post-distribution phase
- Separated by at least 1.5 half-lives
- Allows calculation of individual PK parameters
Interpreting TDM results
Elevated peak:
- May indicate distribution issue
- Verify weight used for dosing
- Consider reducing dose
Elevated trough:
- Extend dosing interval
- Consider reducing dose
- Evaluate renal function
- Higher toxicity risk
Both elevated:
- Likely renal impairment
- Recalculate using current renal function
TDM methods comparison
| Method | Precision | Complexity |
|---|---|---|
| Bayesian + 2 levels | Highest | Requires software |
| PK equations + 2 levels | High | Manual calculation |
| Bayesian + 1 level | Moderate | Requires software |
| Nomogram (Hartford) | Moderate | Simple |
| Threshold interpretation | Lower | Simplest |
Bayesian methods: Incorporate population PK + patient covariates
Practical TDM approach
Day 1: Give loading dose based on weight/renal function
Day 2-3: Draw levels
- If using nomogram: single level at 6-14 hours
- If using PK: peak (30 min post) + trough
Adjust based on results:
- Low peak → Increase dose
- High trough → Extend interval
- Calculate patient-specific parameters
Repeat: Every 3-5 days or with renal function change
Clinical Scenarios
Case 1: Gram-Negative Sepsis
Patient: 72-year-old male, 80 kg, SCr 1.2 mg/dL
Diagnosis: E. coli bacteremia, septic shock
Current therapy: Piperacillin-tazobactam
Question: Should you add an aminoglycoside?
Answer: Consider adding tobramycin or gentamicin
- Septic shock: May benefit from combination
- Short course (3-5 days) minimizes toxicity
- Dose: 7 mg/kg × 80 kg = 560 mg q24h
Case 2: Enterococcal endocarditis
Patient: 55-year-old female, 65 kg, native valve endocarditis
Culture: Enterococcus faecalis, susceptible to ampicillin
Question: What gentamicin regimen?
Answer:
- Check for high-level gentamicin resistance (HLGR-500 µg disk)
- If susceptible: Gentamicin 3 mg/kg/day divided q8h
- Target peak: 3-4 mg/L
- Target trough: < 1 mg/L
- Duration: 4-6 weeks ampicillin, 2 weeks gentamicin
Case 3: Obesity
Patient: 145 kg female, 5’4”, BMI 49
Diagnosis: Pseudomonas pneumonia
Question: How do you dose tobramycin?
Calculation:
- IBW = 45.5 + 2.3(4) = 54.7 kg
- ABW = 54.7 + 0.4(145-54.7) = 54.7 + 36 = 90.7 kg
- Dose = 7 mg/kg × 91 kg = 637 mg → Round to 600 mg q24h
- Obtain levels and adjust
Case 4: Renal impairment
Patient: 70 kg male, CrCl 35 mL/min
Need: Gentamicin for gram-negative coverage
Question: Initial regimen?
Approach:
- Give full loading dose: 7 mg/kg × 70 kg = 490 mg
- Extend interval for maintenance
- CrCl 35 mL/min → Likely q36-48h
- Use Hartford nomogram with 6-14 hour level
- TDM essential - adjust based on levels
Case 5: Cystic fibrosis
Patient: 28-year-old with CF, P. aeruginosa exacerbation
Current weight: 55 kg
Question: Tobramycin dosing considerations?
CF considerations:
- Increased Vd and clearance
- May need 10-12 mg/kg/day
- Higher peaks targeted (20-30 mg/L)
- More frequent monitoring
- Consider inhaled tobramycin for chronic suppression
Inhaled aminoglycosides
Indications:
- Cystic fibrosis (chronic P. aeruginosa)
- VAP (adjunctive therapy)
- NTM pulmonary disease
Formulations:
| Product | Dose | Frequency |
|---|---|---|
| TOBI (tobramycin) | 300 mg | BID, 28 days on/off |
| Tobramycin powder | 112 mg | BID |
| ALIS (amikacin liposome) | 590 mg | Daily |
Key takeaways: Mechanism
- Concentration-dependent bactericidal activity
- Bind to 30S ribosomal subunit
- Cause mistranslation → defective proteins
- Post-antibiotic effect of 3-8 hours
- Synergistic with cell wall-active agents
- AUC/MIC is primary PK/PD driver
Key takeaways: Clinical use
- Primarily for gram-negative infections
- Usually combination therapy
- Extended-interval dosing preferred
- Short courses (3-5 days) when possible
- Reserve for serious infections/MDR organisms
- Plazomicin for CRE
Key takeaways: Dosing
- 5-7 mg/kg q24h (gentamicin/tobramycin)
- 15-20 mg/kg q24h (amikacin)
- Use adjusted body weight in obesity
- Extend interval in renal impairment
- Loading dose independent of renal function
- TDM for courses > 3 days
Key takeaways: Safety
- Nephrotoxicity usually reversible
- Ototoxicity may be permanent
- Target undetectable troughs
- Monitor renal function
- Avoid concurrent nephrotoxins
- Consider genetic screening (MT-RNR1)
Summary: The “Aminoglycoside Checklist”
✓ Is an aminoglycoside appropriate?
✓ Which agent? (Based on organism/susceptibility)
✓ Correct weight for dosing? (ABW if obese)
✓ Renal function assessed?
✓ Drug interactions reviewed?
✓ TDM plan in place?
✓ Expected duration defined? (Keep short!)
✓ Monitoring for toxicity?